Strabismus

Strabismus is a general term referring to ocular misalignment due to extraocular muscle imbalance. In short, the eyes are not straight.
Strabismus occurs in approximately 2% of children under 3 years of age and about 3% of children and young adults. The condition affects males and females equally.
Strabismus has an inherited pattern, i.e., it is much more likely to occur if one or both parents are affected. However, many cases occur without any family history of the disorder.
Strabismus is important to recognize, primarily because, in childhood, it is often associated with the development of amblyopia, or lazy eye. Amblyopia refers to reduced vision, uncorrectable with glasses or contact lenses, due to failure or incomplete development of the visual cortex of the brain.
Strabismus is not only important from the standpoint of amblyopia, however. It is also important for other functional and cosmetic reasons. Strabismus is associated with a reduction of depth perception and if onset is in adulthood, double vision. Furthermore, strabismus presents a cosmetic concern, especially for school-age children.
Treatments for strabismus include spectacles, prism lenses, and surgery aimed at bringing the eyes into proper alignment. Strabismus surgery is done as an outpatient. The procedure involves repositioning the eye muscles (essentially tightening or loosening the muscles) so that the patient’s eyes assume a more normal position.
Presbyopia

Presbyopia is a condition that typically becomes noticeable for most people around age 45. In children and young adults, the lens inside the eye can easily focus on distant and near objects. With age, the lens loses its ability to focus adequately.
Although presbyopia is not completely understood, it is thought that the lens and its supporting structures lose the ability to make the lens longer during close vision effort.
To compensate, affected individuals usually find that holding reading material further away makes the image clearer. Ultimately, aids such as reading glasses are typically needed by the mid-forties.
Besides glasses, presbyopia can be dealt with in a number of ways. Options include monovision and multifocal contact lenses, monovision laser vision correction, and new presbyopia correcting implant lenses.
Myopia (Nearsightedness)
Nearsighted individuals typically have problems seeing well at a distance and are forced to wear glasses or contact lenses.
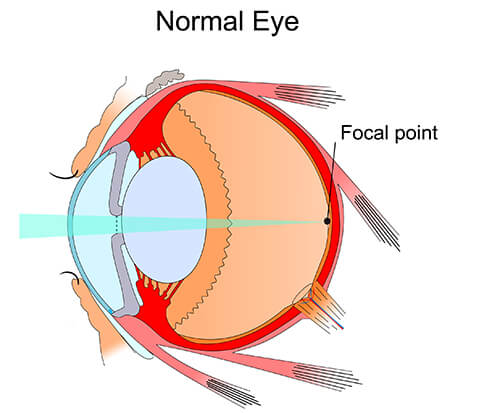
The nearsighted eye is usually longer than a normal eye, and its cornea may also be steeper. Therefore, when light passes through the cornea and lens, it is focused in front of the retina. This will make distant images appear blurred.
There are several refractive surgery solutions available to correct nearly all levels of nearsightedness.
Hyperopia (Farsightedness)

Farsighted individuals typically develop problems reading up close before the age of 40. The farsighted eye is usually slightly shorter than a normal eye and may have a flatter cornea. Thus, the light of distant objects focuses behind the retina unless the natural lens can compensate fully.
Near objects require even greater focusing power to be seen clearly and therefore, blur more easily.
LASIK, Refractive Lens Exchange, and Contact lenses are a few of the options available to correct farsightedness.
Astigmatism
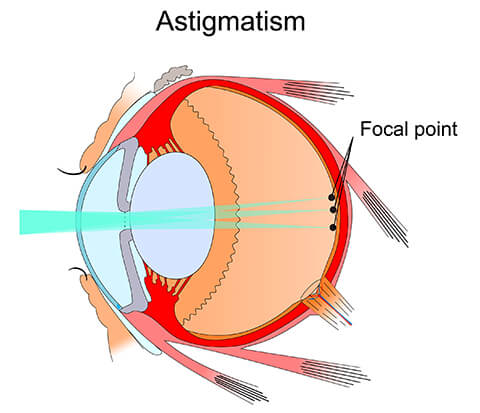
Asymmetric steepening of the cornea or natural lens causes light to be focused unevenly, which is the main optical problem in astigmatism. To individuals with uncorrected astigmatism, images may look blurry or shadowed. Astigmatism can accompany any form of refractive error and is very common.
Astigmatism can be corrected with glasses, contact lenses, corneal relaxing incisions, laser vision correction, and special implant lenses.
Many individuals with myopia or hyperopia also have some degree of astigmatism. People with significant astigmatism experience blurred or distorted vision for all objects, whether near or far. Astigmatism means that your cornea, instead of being spherical like the side of a basketball, is slightly oval, shaped more like the side of a football.
Your cornea is more curved in one direction than the other. As a result, light rays entering the eye from different points on the cornea’s surface are bent irregularly and are focused at several different points, rather than meeting at just one focal point. Almost everyone has a small degree of astigmatism.
While LASIK is the most common procedure used for astigmatism correction, for some astigmatism patients other techniques are more appropriate. For example, for astigmatism patients undergoing lens implant surgery (during cataract surgery or refractive lens exchange, for example), a simple procedure called Astigmatic Keratotomy can be performed simultaneously to reduce or eliminate low to moderate levels of astigmatism.
Astigmatism Correction
ASTIGMATIC KERATOTOMY or Limbal Relaxing Incisions (AK or LRIs)
Astigmatism can be corrected by small, accurate incisions on the surface of the outer cornea. AK (and LRIs) is a safe and effective treatment for patients with pure astigmatism (no coexisting nearsightedness or farsightedness) and can be done in an office setting. The small incisions are placed in the steep portion of the patient’s cornea as a means of allowing that area to relax, or flatten. The result is a more spherical and properly shaped cornea.
The most common application of AK is for the correction of astigmatism at the time of any Lens Implant surgery (including cataract, Refractive Lens Exchange, or Implantable Contact Lens procedures). Astigmatic Keratotomy (AK) patients enjoy rapid visual recovery and an improvement in both distance and near vision. For higher amounts of astigmatism, LRIs can be combined with astigmatism correcting lens implants (toric IOLs).
Astigmatism Correction Conclusions
If you are not a candidate for Astigmatic Keratotomy or Limbal Relaxing Incisions but are still bothered by visual distortions caused by astigmatism you may still be a candidate for other astigmatism correcting techniques such as LASIK or surface ablation.
